




The land has always been etched into the Australian identity. Revered by its original inhabitants and a source of inspiration for poets and rock stars, only recently has its contamination and its loss from soil erosion made headlines. While our national anthem extols our "golden soil", there is no mention of the high arsenic levels sometimes associated with gold deposits.
Soil contamination was largely ignored until the 1980s, when both regional contamination (around places such as Port Pirie, site of the world's largest lead smelter) and localised contamination (such as at cattle tick dip sites in Queensland and New South Wales), were recognised. Significantly elevated blood lead levels and subtle cognitive effects in children were detected in Port Pirie,1 while exposure to pesticides, especially arsenic and DDT, was of concern near cattle tick dip sites.2
At the same time, urban consolidation was creating pressure to transform old inner-city industrial sites into residential areas. Bank foreclosures occurred on properties that then became onerous possessions because of contamination liabilities. This led to audits becoming part of transactions involving industrial land, the identification of many contaminated sites and, in the 1990s, the development of national guidelines3,4 for assessing and managing contaminated sites in Australia and New Zealand.
There have been relatively few epidemiological studies, in Australia or overseas, of health effects related to contaminated sites. A UK study5 of people living within a two-kilometre radius of a landfill (80% of the UK population falls into this category) detected increased risks of congenital anomalies and low birthweight. However, the study did not differentiate potential data artefacts and confounding effects from possible causal associations. Moreover, such studies often do not identify actual exposure pathways.
Little is known about the scale of soil contamination in Australia because of limited investigation and definitional issues. One estimate, based on extrapolation from Queensland data, is that there may be as many as 200 000 contaminated sites in Australia (a few examples are shown in Box 1).6
The amount of contaminated material can be considerable: at Port Pirie, where a smelter has operated since 1889, it is estimated that 80 000 tonnes of lead have been deposited on land and almost 90 000 tonnes in the marine environment.7 Elevated lead concentrations have been detected in soil as far as 60 km downwind of the smelter.8
The most common toxic soil contaminants are lead (eg, from paint, scrapyards), arsenic (eg, from agricultural pesticides, weed clearance and tanneries), BTEX (benzene, toluene, ethylbenzene and xylenes from petroleum products), polycyclic aromatic hydrocarbons (eg, from combustion products, tars and gasworks) and persistent pesticides (eg, DDT used in cattle tick dips). At sufficient exposures, the first significant health effects noted from lead are cognitive effects, while other contaminants such as arsenic, benzene and some polycyclic aromatic hydrocarbons are regarded as carcinogens.
Many contaminants do not cause obvious soil discoloration unless they are in very high concentrations. There may, instead, be subtle signs of contamination, such as reduced or absent plant growth. Some sites have been identified by odour or by sickness in animals. For example, in the 1950s, cows belonging to the mayor of Murray Bridge, grazing under the bridge for which the city was named, were poisoned by lead from paint released by sanding and scraping of the bridge during routine maintenance.9 In the 1980s, an Adelaide backyard contaminated in the past by lead sinker manufacture was identified after a vet diagnosed lead poisoning in a dog (Len Turczynowicz, Scientific Officer [toxicologist], South Australian Department of Human Services, personal communication).
Soil sampling may be performed at random locations, at regular spacings, or where contamination is thought to be most likely because of the site history — or using a combination of these approaches. Sampling is usually undertaken at different depths. As contamination concentrations often vary greatly across a site, isolated "hot spots" may be missed or randomly oversampled by the use of a grid.
Potential exposures are greater where there is regional, not just localised, contamination, as more exposure opportunities exist — at home, at childcare or shopping centres, and more generally from contaminated air, food and water.
Direct soil ingestion is usually the principal exposure route. People rarely deliberately consume "dirt", but children often convey dirt to the mouth on their hands, and adults may ingest contaminated soil on vegetables or on the surface of cigarettes.
Children are the "key receptor" because of hand-to-mouth behaviours and because gastrointestinal absorption of heavy metals is higher in children than adults. Furthermore, children have heightened susceptibility to the effects of heavy metals because of their developing neurobehavioural system.
It is difficult to measure soil ingestion accurately. One surrogate measure is based on subtracting the quantity of tracer elements ingested in food from faecal amounts of the tracers. Children aged between one and four years living at a contaminated site in Montana, USA, have been estimated to ingest a median of 17 mg of soil per day.10 Peak soil ingestion probably occurs around 15–24 months of age.1 The condition of soil pica (the recurrent ingestion of unusually high amounts of soil) is considered to occur rarely in Australia, but may result in high soil ingestion by certain individuals. In some countries there is cultural geophagia.
Contamination of homegrown fruit, vegetables and herbs is a common concern of people living on or near contaminated sites.11 There are substantial differences in uptake of contaminants according to the type of contaminant and the species of plant. Cadmium is taken up more readily than lead, but lead may still adhere to the dust on green leafy vegetables.
Dust arising from the site may cause concerns about contamination of rainwater tanks, and measures to test rainwater and prevent contamination may be warranted.
If a patient presents with concerns about exposure to toxic substances from a contaminated site, the following questions should be considered:
Environmental protection agencies, public health departments and local governments may be able to provide useful information in this regard (see case study in Box 2).
A key principle is to identify exposure pathways and try to prevent or minimise further exposure. For example, in an environment with high lead contamination, doctors should also check for iron deficiency and establish whether pregnant women are receiving adequate calcium12 (calcium competes with lead for absorption and retention). If indicated, children should be referred for neurodevelopmental and behavioural assessment. Detailed recommended interventions for various concentrations of elevated blood lead are available,13 and may include paediatric assessment, environmental assessment and sampling (if the source is not obvious), and remediation. A large randomised controlled trial14 concluded that chelation therapy was not indicated for children with blood lead concentrations below 45 μg/dL, as these children did not perform better in tests of cognition, behaviour and neuropsychological function after chelation therapy.
To determine the need for intervention, the risk from a contaminated site needs to be assessed (Box 3).
For sites with localised contamination, interventions should be directed at remediating the site. Where there is regional contamination, environmental management will also need to focus on controlling air, food and water contamination and minimising contamination of living areas and children's play areas. Large mats at external doors can reduce the amount of soil being carried into houses on footwear, and wet mopping and carpet cleaning can reduce the burden in living areas. Using a standard vacuum cleaner can paradoxically worsen exposures, as the fine particulate fraction that will pass through the filter and be blown back into the surrounding environment will often contain a disproportionately high level of the contaminant. A vacuum cleaner with a HEPA (high efficiency particulate arresting) filter is preferred.
Environmental agencies have primary legislative responsibility for the assessment and management of contaminated sites. Importantly, this is underpinned by a range of State and Federal powers (eg, National Environment Protection Measures) that control the production, storage and disposal of waste and are designed to prevent further contamination.
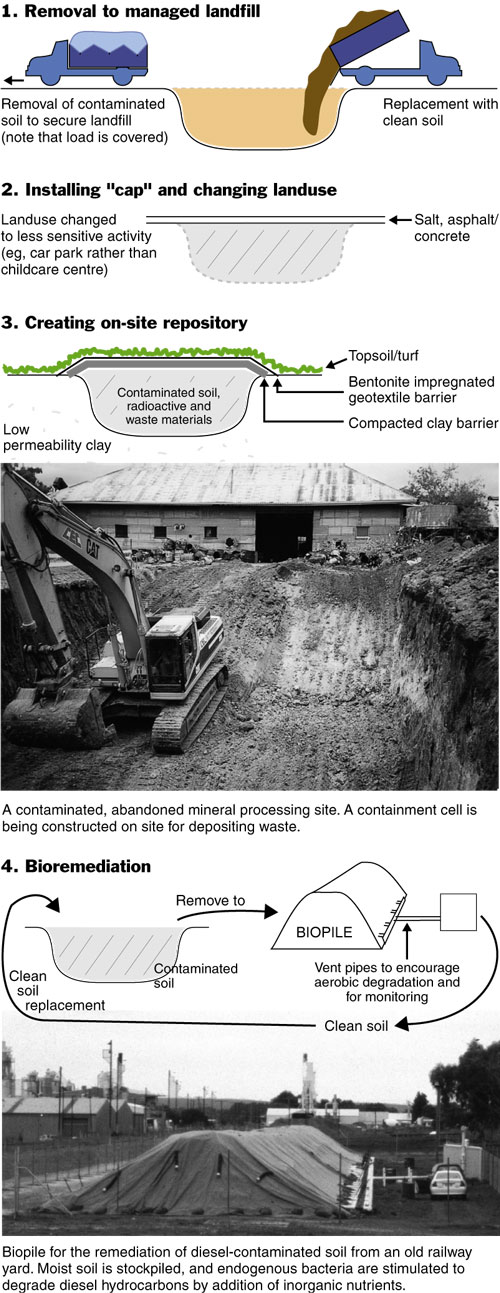
Large sites with extensive contamination (including gasworks, railway yards and landfills) have been successfully remediated to enable safe use. The Sydney Olympics site at Homebush Bay, where a variety of methods were used (including clean soil capping over mounds of contaminated soil), is an example of large-scale remediation.
It has been more difficult to remediate contaminated groundwater that has often arisen from leaking underground storage tanks containing petroleum products. Contaminated groundwater plumes have in some instances extended a considerable distance off site. In these situations, benzene has often been the principal concern because of its ability to rapidly disperse in aquifers and its carcinogenicity.
The conventional approaches to remediating contaminated sites are shown in Box 4. Novel clean-up methods are also being considered. One involves growing crops that will bioaccumulate heavy metals from the soil — the crops can then be harvested and the contaminant extracted from them. Another is vitrification: an electric arc is generated between large buried electrodes, creating temperatures sufficient to turn the soil and its contaminants into a glass-like mass from which the contaminants cannot leach. This very expensive method has been used at the nuclear testing site of Maralinga.
Unfortunately, the high cost of remediation and the difficulty of identifying responsible parties have sometimes resulted in the persistence of unremediated wastelands.
In the coming years, we will refine our assessment and management of soil contamination and associated health risks (Box 5).
To minimise further loss of clean soil in the future, we must learn to treat it as a precious and limited resource and develop and apply improved legislative tools that will help to achieve this end.
3: How risky is a site?
Precise estimates of the hazard risk of a contaminated site are often made, usually based on US Environmental Protection Agency (EPA) methodologies. However, quantitative estimates may be misleading15 because of uncertainties arising from soil sampling processes and from exposure and toxicological assessments. These estimates have been particularly controversial in cases where the soil contaminants are classified as carcinogenic.
To address these problems, Australia has developed an approach to the environmental and health risk assessment of sites,4 a method for assessing carcinogenic soil contaminants,16 and environmental health risk assessment guidelines.15 The guidelines set out five stages of investigation:
Issue identification, to establish where risk assessment is of value;
Hazard identification, to determine possible adverse effects;
Dose–response assessment, to estimate the incidence of adverse effects at different exposure levels;
Exposure assessment, to estimate the contributions of various exposure pathways to total population exposures; and
Risk characterisation, to provide a qualitative and/or quantitative estimate of the nature, severity and potential incidence of effects in a population.15
4: Remediation of contaminated sites
The principal approaches to remediating contaminated sites are:
5: Reflections and predictions
Circa 1900
Natural "contamination" arising from alluvial deposits of some minerals (eg, arsenic in goldmining areas of Victoria; lead in Broken Hill) often exacerbated by mining and smelting operations.
Older inner-city areas contaminated from many sources (eg, use of industrial waste for land reclamation; industrial debris from foundries, gasworks, incinerators, leaking underground storage tanks and flaking lead-based paints).
Role of lead-based paint in childhood lead poisoning first recognised around this time. Turner (1897) related lead poisoning to habitation and Gibson (1904) identified source as paint on railings and walls.17
Rural areas contaminated by use of persistent pesticides (eg, lead arsenate in orchards; arsenic in cattle dips).
Circa 2100 (an optimistic view)
Uncontaminated soil has become highly valued by the community. There is greater concern about contamination, with more stringent laws to control it.
Contaminated sites have been identified and clearly mapped.
Three-dimensional methods of site characterisation and new technologies allow contaminants to be extracted or degraded more accurately and efficiently, rather than retained in landfills.
More accurate health-risk assessments allow better estimates of risk and better management of sites.
Site characterisation, risk assessment and site remediation remain challenging and expensive.
Increasing urban density, smaller block sizes and extensive paving mean that city dwellers have little exposure to soil.
- Andrew J Langley1
- Central Public Health Unit Network, Queensland Health, Maroochydore, QLD.
Greg O'Brien (Environmental Protection Agency, QLD) provided valuable advice and illustrations, Nick McClure (Flinders University, SA) provided illustrations, and Cathy Phipps (Environmental Health Centre, Port Pirie) provided valuable information.
None identified.
- 1. Tong S, Baghurst P, McMichael A, et al. Lifetime exposure to environmental lead and children's intelligence at 11–13 years: the Port Pirie cohort study. BMJ 1996; 312: 1569-1575.
- 2. Beard J. The evaluation of DDT contaminated soil associated with cattle tick dip sites. In: Langley A, van Alphen M, editors. The health risk assessment and management of contaminated sites. Contaminated Sites Monograph Series. No. 2. Adelaide: South Australian Health Commission, 1993: 119-133.
- 3. Australian and New Zealand guidelines for the assessment and management of contaminated sites. Canberra: Australian and New Zealand Environment and Conservation Council and National Health and Medical Research Council, 1992.
- 4. National environment protection measure for the assessment of site contamination. Adelaide: National Environment Protection Council, 1999.
- 5. Elliott P, Briggs D, Morris S, et al. Risk of adverse birth outcomes in populations living near landfill sites. BMJ 2001; 323: 363-368.
- 6. Assessment of site contamination. Impact statement. Adelaide: National Environment Protection Council, 1999.
- 7. Body PE, Inglis GR, Mulcahy DE. Lead contamination in Port Pirie. SADEP Report Number 101. Adelaide: Department of Environment and Planning, 1988.
- 8. Tiller KG. Determining background levels. In: El Saadi O, Langley A, editors. The health risk assessment and management of contaminated sites. Adelaide: South Australian Health Commission, 1991: 98-101.
- 9. Woodruff P. Two million South Australians. Kent Town, SA: Peacock Publications, 1984.
- 10. Stanek EJ, Calabrese EJ. Daily soil ingestion estimates for children at a Superfund site. Risk Anal 2000; 20: 627-635.
- 11. Cross SJ, Taylor ER. Human exposure to soil contaminants through the consumption of home-grown produce. Contaminated Sites Monograph Series. No 6. Adelaide: South Australian Health Commission, 1996.
- 12. Clinical support in Port Pirie. Port Pirie: Environmental Health Centre, [undated].
- 13. Alperstein G, Taylor R, Vimpani G. Lead alert: a guide for health professionals. Canberra: Commonwealth Environment Protection Agency, 1994.
- 14. Rogan WJ, Dietrich KN, Ware JH, et al. The effect of chelation therapy with succimer on neuropsychological development on children exposed to lead. N Engl J Med 2001; 344: 1421-1426.
- 15. enHealth. Environmental health risk assessment. Guidelines for assessing human health risks from environmental hazards. Canberra: Department of Health and Ageing, 2002.
- 16. Toxicity assessment guidelines for carcinogenic soil contaminants. Canberra: National Health and Medical Research Council, 1999.
- 17. Christophers A. Paediatric lead poisoning in Queensland. How and why it was so different from lead poisoning elsewhere. Melbourne: Monash University Medical School, 1999.
Abstract
There are many contaminated soil sites in Australia.
Contamination may be from human activities (eg, smelters, industrial waste dumps, old gasworks) or from naturally occurring sources (eg, surface mineralisation).
Concentrations of contaminants may vary markedly across a site. Their distribution may be localised or quite extensive.
Common contaminants include lead, arsenic, cadmium, petrol and diesel products, and polycyclic aromatic hydrocarbons.
People living on or near a contaminated site will often be concerned about potential effects on their health. Assessing their exposure potential and/or measuring levels of biological markers often allays concerns, but occasionally confirms them (eg, elevated blood lead levels and subtle cognitive effects have been found in some people living near the Port Pirie lead smelter).