





Adolescent e‐cigarette use (vaping) and its harms are public health concerns.1 A national survey in 2019 found that 10% of 14–17‐year‐old Australians had used e‐cigarettes.2 More recent studies, smaller or non‐representative, have suggested that the rate is rapidly increasing.3,4 Little is known about how e‐cigarette use varies by socio‐demographic factors, such as gender, socio‐economic status, and residential remoteness.
We assessed the prevalence and patterns of e‐cigarette use, and socio‐demographic features of Australian adolescents who participated in the 36‐month post‐baseline assessment of the Health4Life cluster randomised controlled trial.5 During 1 July – 31 December 2022, 4445 students aged 14–17 years from 70 schools in New South Wales, Queensland, and Western Australia (67% of 6640 baseline participants) were invited to complete an online survey on e‐cigarette use as part of the Health4Life assessment. We estimated the proportions of participants who reported using e‐cigarettes ever, during the past twelve months, during the preceding 30 days, and regularly (past 30 days and at least weekly); the prevalence of use during the past twelve months and of current regular use was also estimated by gender, remoteness, and relative socio‐economic status in logistic regression analyses. To overcome the constraints associated with odds ratios for frequently occurring outcomes, we used prevalence ratios (PRs) with 95% confidence intervals (CIs), adjusted for all covariates and school‐level clustering. The University of Sydney (2018/882), the University of Queensland (2019000037), and Curtin University (HRE2019‐0083) human research ethics committees approved the Health4Life study; the study was also approved under the NSW State Education Research Applications Process (2019006) and by the Catholic Education Diocese of Bathurst, the Catholic Schools Office Diocese of Maitland–Newcastle, Edmund Rice Education Australia, the Brisbane Catholic Education Committee (373), and Catholic Education Western Australia (RP2019/07).
The mean age of the 4204 students who provided full responses to the e‐cigarette survey (95% response rate) was 15.7 years (standard deviation [SD], 0.6 years); 2034 were girls (48.5%) (Box 1). A total of 1094 of 4204 respondents reported ever having used e‐cigarettes (26.0%; 95% CI, 24.8–27.4%); mean age at first use was 14.0 years (SD, 1.3 years). E‐cigarette use in the past twelve months was reported by 858 of 4204 respondents (20.4%; 95% CI, 19.2–21.7%), current use by 423 of 4204 (10.1%; 95% CI, 9.2–11.0%), and current regular use by 240 of 4204 (5.7%; 95% CI, 5.1–6.5%).
The prevalence of use in the past twelve months was higher for boys (PR, 1.55; 95% CI, 1.33–1.80) and non‐binary participants (PR, 1.67; 95% CI, 1.22–2.29) than for girls. The prevalence of current regular use was higher for non‐binary participants (PR, 1.88; 95% CI, 1.03–3.44) and those who preferred to not report gender (PR, 2.09; 95% CI, 1.01–4.34) than for girls. Socio‐economic status and remoteness did not influence prevalence of current use or use in the past twelve months (Box 2).
Although our survey was one of the largest of e‐cigarette use by young people in Australia and was not subject to parental influence of responses, our non‐probabilistic sample means that extrapolation of our findings to all Australian adolescents should be cautious, especially as it included young people from only three states, and large proportions from independent schools and major cities.
Our findings indicate that strategies for preventing the uptake and reducing the use of e‐cigarettes by Australian adolescents are needed. A multilevel approach with components at the individual (eg, primary health care screening and intervention), school (eg. normative education and resistance skills training), and community levels (eg, e‐cigarette control policies, media campaigns) would be appropriate.
Box 1 – Socio‐demographic characteristics of the 4204 students aged 14–17 years who provided full responses to the e‐cigarette survey in the Health4Life 36‐month post‐baseline assessment
|
Characteristic |
Students |
Proportion (95% CI) |
|||||||||||||
|
|
|||||||||||||||
|
Age (years), mean (SD) |
15.7 (0.6) |
— |
|||||||||||||
|
Gender |
|
|
|||||||||||||
|
Girls |
2034 |
48.5% (47.0–50.0%) |
|||||||||||||
|
Boys |
1976 |
47.1% (45.6–48.6%) |
|||||||||||||
|
Non‐binary |
114 |
2.7% (2.3–3.3%) |
|||||||||||||
|
Prefer not to say |
71 |
1.7% (1.3–2.1%) |
|||||||||||||
|
Missing data |
9 |
— |
|||||||||||||
|
State |
|
|
|||||||||||||
|
New South Wales (37 schools) |
2263 |
53.8% (52.3–55.3%) |
|||||||||||||
|
Queensland (18 schools) |
1163 |
27.7% (26.3–29.0%) |
|||||||||||||
|
Western Australia (16 schools) |
778 |
18.5% (17.4–19.7%) |
|||||||||||||
|
School type |
|
|
|||||||||||||
|
Independent (37 schools) |
2188 |
52.0% (50.5–53.6%) |
|||||||||||||
|
Catholic (10 schools) |
775 |
18.4% (17.3–19.6%) |
|||||||||||||
|
Government (24 schools) |
1241 |
29.5% (28.2–30.9%) |
|||||||||||||
|
Socio‐economic status* |
|
|
|||||||||||||
|
Lower (< 0.20) |
720 |
17.8% (16.6–19.0%) |
|||||||||||||
|
Middle (0.20–0.79) |
2802 |
69.2% (67.8–70.6%) |
|||||||||||||
|
Upper (0.80–1.0) |
526 |
13.0% (12.0–14.1%) |
|||||||||||||
|
Missing data |
156 |
— |
|||||||||||||
|
Remoteness† |
|
|
|||||||||||||
|
Inner or outer regional |
363 |
8.6% (7.8–9.5%) |
|||||||||||||
|
Major city |
3841 |
91.4% (90.5–92.2%) |
|||||||||||||
|
|
|||||||||||||||
|
CI = confidence interval; SD = standard deviation. * Family Affluence Scale III scores (based on family owning a car, the adolescent having their own bedroom, and frequency of away‐from‐home vacations in preceding year6) were converted to ridit scores to compare socio‐economic status with other students in the study. † Australian Statistical Geography Standard.7 |
|||||||||||||||
Box 2 – E‐cigarette use during the past twelve months and current regular e‐cigarette use among 14–17‐year‐old students who participated in the Health4Life 36‐month post‐baseline survey, by socio‐demographic characteristics
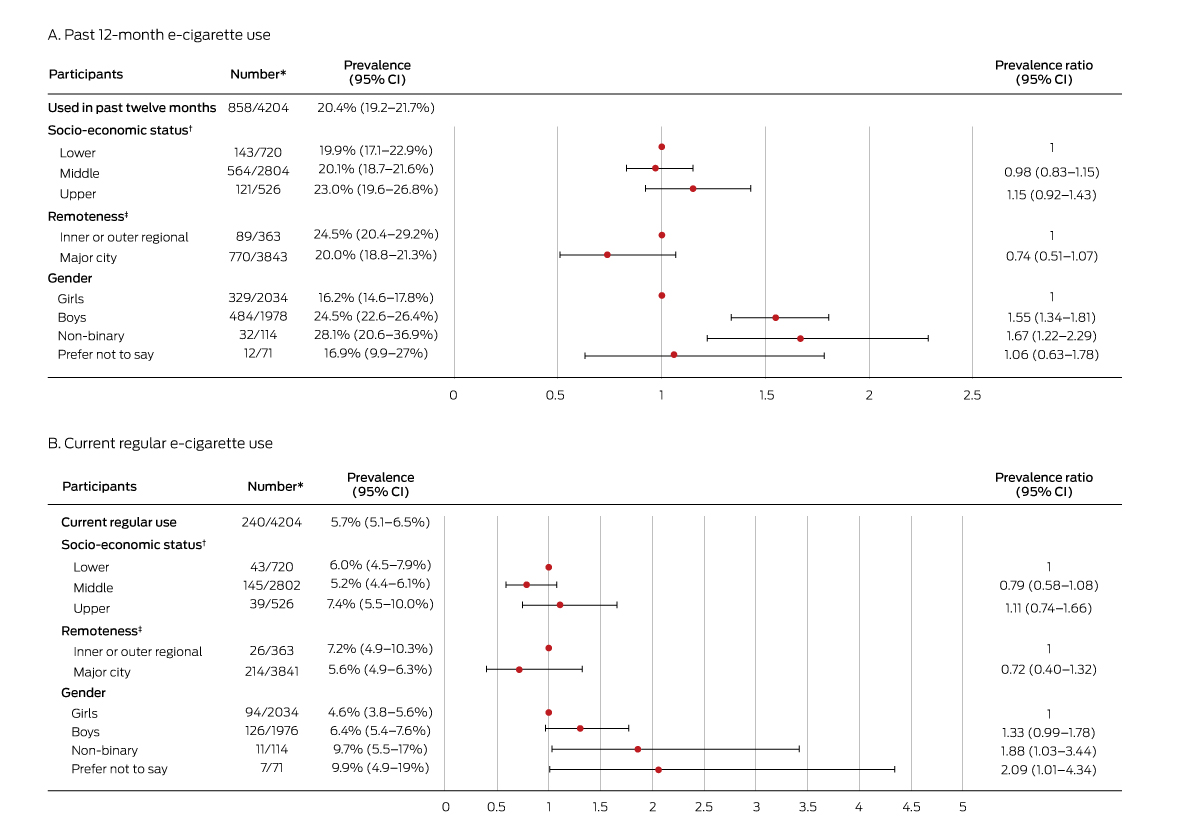
CI = confidence interval. * Number of respondents who used e‐cigarettes during time period/total number of respondents. † Family Affluence Scale III scores (based on family owning a car, the adolescent having their own bedroom, and frequency of away‐from‐home vacations in preceding year6) were converted to ridit scores to compare socio‐economic status with other students in the study. ‡ Australian Statistical Geography Standard.7
Received 5 May 2023, accepted 17 July 2023
- 1. Banks E, Yazidjoglou A, Brown S, et al. Electronic cigarettes and health outcomes: umbrella and systematic review of the global evidence. Med J Aust 2023; 218: 267‐275. https://www.mja.com.au/journal/2023/218/6/electronic‐cigarettes‐and‐health‐outcomes‐umbrella‐and‐systematic‐review‐global
- 2. Australian Institute of Health and Welfare. National Drug Strategy Household Survey 2019 (Cat. no. PHE 270). 16 July 2020. https://www.aihw.gov.au/reports/illicit‐use‐of‐drugs/national‐drug‐strategy‐household‐survey‐2019/contents/summary (viewed Mar 2023).
- 3. Watts C, Egger S, Dessaix A, et al. Vaping product access and use among 14–17‐year‐olds in New South Wales: a cross‐sectional study. Aust N Z J Public Health 2022; 46: 814‐820.
- 4. Wakefield M, Haynes A, Tabbakh T, et al. Current vaping and current smoking in the Australian population aged 14+ years: February 2018 – March 2023. Report for the Australian Department of Health and Aged Care. May 2023; updated June 2023. https://www.health.gov.au/resources/publications/current‐vaping‐and‐smoking‐in‐the‐australian‐population‐aged‐14‐years‐or‐older‐february‐2018‐to‐march‐2023?language=en (viewed June 2023).
- 5. Teesson M, Champion KE, Newton NC, et al; Health4Life Team. Study protocol of the Health4Life Initiative: a cluster randomised controlled trial of an eHealth school‐based program targeting multiple lifestyle risk behaviours among young Australians. BMJ Open 2020; 10: e035662.
- 6. Torsheim T, Currie C, Boyce W, et al. Material deprivation and self‐rated health: a multilevel study of adolescents from 22 European and North American countries. Soc Sci Med 2004; 59: 1‐12.
- 7. Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS), volume 5: remoteness structure (1270.0.55.005), July 2016. Updated 16 Mar 2018. https://www.abs.gov.au/ausstats/abs@.nsf/mf/1270.0.55.005 (viewed June 2023).
- 1. Banks E, Yazidjoglou A, Brown S, et al. Electronic cigarettes and health outcomes: umbrella and systematic review of the global evidence. Med J Aust 2023; 218: 267‐275. https://www.mja.com.au/journal/2023/218/6/electronic‐cigarettes‐and‐health‐outcomes‐umbrella‐and‐systematic‐review‐global
- 2. Australian Institute of Health and Welfare. National Drug Strategy Household Survey 2019 (Cat. no. PHE 270). 16 July 2020. https://www.aihw.gov.au/reports/illicit‐use‐of‐drugs/national‐drug‐strategy‐household‐survey‐2019/contents/summary (viewed Mar 2023).
- 3. Watts C, Egger S, Dessaix A, et al. Vaping product access and use among 14–17‐year‐olds in New South Wales: a cross‐sectional study. Aust N Z J Public Health 2022; 46: 814‐820.
- 4. Wakefield M, Haynes A, Tabbakh T, et al. Current vaping and current smoking in the Australian population aged 14+ years: February 2018 – March 2023. Report for the Australian Department of Health and Aged Care. May 2023; updated June 2023. https://www.health.gov.au/resources/publications/current‐vaping‐and‐smoking‐in‐the‐australian‐population‐aged‐14‐years‐or‐older‐february‐2018‐to‐march‐2023?language=en (viewed June 2023).
- 5. Teesson M, Champion KE, Newton NC, et al; Health4Life Team. Study protocol of the Health4Life Initiative: a cluster randomised controlled trial of an eHealth school‐based program targeting multiple lifestyle risk behaviours among young Australians. BMJ Open 2020; 10: e035662.
- 6. Torsheim T, Currie C, Boyce W, et al. Material deprivation and self‐rated health: a multilevel study of adolescents from 22 European and North American countries. Soc Sci Med 2004; 59: 1‐12.
- 7. Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS), volume 5: remoteness structure (1270.0.55.005), July 2016. Updated 16 Mar 2018. https://www.abs.gov.au/ausstats/abs@.nsf/mf/1270.0.55.005 (viewed June 2023).
Open access:
Open access publishing facilitated by The University of Sydney, as part of the Wiley – The University of Sydney agreement via the Council of Australian University Librarians.
The Health4Life study was funded by the Paul Ramsay Foundation and the National Health and Medical Research Council (NHMRC; Centre of Research Excellence in the Prevention and Early Intervention in Mental Illness and Substance Use [PREMISE]: APP11349009). Katrina Champion (APP1120641), Maree Teesson (APP1078407), and Nicola Newton (APP1166377) are supported by NHMRC fellowships. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The Health4Life study was led by researchers at the Matilda Centre at the University of Sydney, Curtin University, the University of Queensland, the University of Newcastle, Northwestern University, and UNSW Sydney. We acknowledge all the investigators and research staff who have worked on the study, as well as the participating schools, students, and teachers. The research team also acknowledges the assistance of the New South Wales Department of Education, the Catholic Education Diocese of Bathurst, the Catholic Schools Office Diocese of Maitland–Newcastle, Edmund Rice Education Australia, the Brisbane Catholic Education Committee, and Catholic Education Western Australia for access to their schools.
No relevant disclosures.