





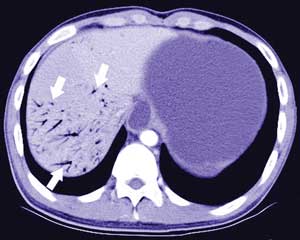
A 17-year-old man with a slim build presented with recurrent postprandial epigastric fullness and bilious vomiting. He was acutely unwell. An abdominal radiograph showed gastric and duodenal distension. Contrast computed tomography scans showed proximal duodenal dilatation (Box, A, arrow), with a triangular-shaped duodenum, extensive hepatic portal venous gas (Box, B, arrows), and a massively distended stomach.
Superior mesenteric artery syndrome with hepatic portal venous gas was diagnosed. This syndrome occurs when the fat pad between the superior mesenteric artery and its origin at the aorta is lost, causing a sharp, narrow angle at the aortomesentery junction. The third portion of the duodenum is compressed and becomes obstructed when passing through this angle.1 Hepatic portal venous gas can develop as a result of bowel ischaemia.
Surgical therapy with duodenojejunostomy is the treatment of choice for a severely ill patient, or when more conservative treatment has failed.2
- Chi-Lun Tsai1
- Ming-Jenn Chen2
- Che-Kim Tan3
- Khee-Siang Chan4
- Kuo-Chen Cheng5
- Chi-Mei Medical Center, Yungkang City, Tainan County, Taiwan.
- 1. Cohen LB, Field SP, Sachar DB. The superior mesenteric artery syndrome. The disease that isn’t, or is it? J Clin Gastroenterol 1985; 7: 113-116.
- 2. Ylinen P, Kinnunen J, Hockerstedt K. Superior mesenteric artery syndrome. A follow-up study of 16 operated patients. J Clin Gastroenterol 1989; 11: 386-391.